RGCIRC Team
Breast Cancer
27 November, 2023
Breast Cancer
There are striking disparities in global cancer burden in women regarding current cancer volumes, trends, risk factors, prevention, early detection and survivorship.
According to WHO, Breast Cancer is the second most common cancer in the world and most frequent cancer among women, impacting over 1.5 million women each year. It also causes the greatest number of cancer-related deaths among women. In 2015, 570,000 women died from breast cancer – that is approximately 15% of all cancer deaths among women.
Breast cancer rates are higher among women in more developed countries and rates and are increasing in nearly every region globally.
Breast cancer has ranked number one cancer among Indian females with age adjusted rate as high as 25.8 per 100,000 women and mortality 12.7 per 100,000 women. Breast cancer projection for India during time periods 2020 suggests the number to go as high as 1797900.
Throughout her lifetime, a woman has a 1 in 8 risk of developing breast cancer. No matter what your age you need to be aware of risk factors. In many cases of breast cancer early diagnosis is the key to survival.
Breast cancer is a global disease (25% new cancer diagnoses)and is most common cancer in women in world. In India following facts are worrisome:
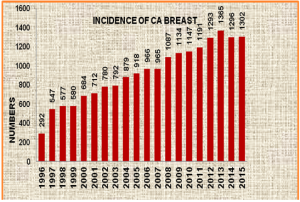
Fig. 1
Rajiv Gandhi Cancer Institute and Research Center (RGCIRC) is a premium tertiary Cancer Institute of Northern India. The number of malignant breast cancer cases registered with RGCIRC, Fig.1 is showing a rising trend as the numbers are rising in the country.
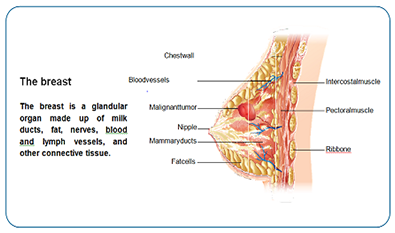
Breast cancer starts when cells in the breast begin to grow out of control. These cells usually form a tumor that can often be seen on imaging -ultrasonography or mammography or felt as a lump. The tumor is malignant (cancer) if the cells can grow into (invade) surrounding tissues or spread (metastasize) to distant areas of the body. Breast cancer occurs mostly in women, but men can get breast cancer, too (1%).
Breast cancers can develop in any part of the breast. Most breast cancers begin in the ducts that carry milk to the nipple (ductal cancers). Some start in the glands that make breast milk (lobular cancers). Lesser common types of breast cancer are sarcomas and lymphomas.

Credit: Terese Winslow LLC/National Cancer Institute
Fig 2
Usually breast cancer presents as a painless lump in the breast which rapidly increases in size.It may also present as a painful lump,a change in breast size and shape ,skin dimpling, thickening ,eczematous changes, redness, recent nipple inversion or abnormalities(ulceration,retraction or bloody discharge) and axillary lump.Some breast cancers are detected on screening mammograms at an earlier stage, often before they can be felt, and before symptoms develop.Usually 80% breast lumps are benign and not cancer (malignant). But some breast lumps can increase a woman’s risk of getting breast cancer. Any breast lump or change in overlying skin needs to be checked by a health care professional to rule out malignancy.
Causes
The causes of breast cancer aren’t fully understood, making it difficult to say why one woman may develop breast cancer and another may not. The universal truth is that breast cancer is always caused by damage to a cell’s DNA.
However, there are risk factors known to affect the likelihood of developing breast cancer. Some of these can be modified while some cannot.
The risk of developing breast cancer increases with age. The most common age group among women being in the postmenopausal and fifth decade. The table below depicts the same fact with respect to the breast cancer patients registered with RGCIRC.
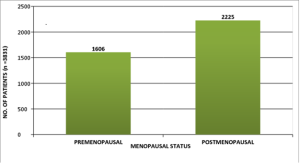
Fig.3
All women who are 50 to 70 years of age should be screened for breast cancer every two years.
With a positive family history there is a higher risk of developing breast cancer. However, because breast cancer is the most common cancer in women, it’s possible for it to occur in more than one family member by chance also.
Approximately 5-10% breast cancers are hereditary. The genes known as BRCA1 and BRCA2 may increase the risk of developing both breast and ovarian cancer. These genes are passed on from a parent to their siblings.
If there are two or more close relatives from the same side of the family – such as mother, sister or daughter – who have had breast cancer under the age of 50, then the candidate becomes eligible for surveillance for breast cancer, or genetic screening and counselling to determine risk status.
If there is a breast cancer or early non-invasive cancer cell changes in breast ducts, there is a higher risk of developing it again, either in the same breast or in the other breast.
A benign breast lump doesn’t mean you have breast cancer, but certain types of lump may also slightly increase your risk of developing it.
Certain benign changes in your breast tissue, such as cells growing abnormally in ducts (atypical ductal hyperplasia), or abnormal cells inside your breast lobes (lobular carcinoma in situ), can make getting breast cancer more likely.
Women with dense breast tissue may have a higher risk of developing breast cancer as there are more cells that can become cancerous. Dense breast tissue can also make a breast scan (mammogram) difficult to read, as any lumps or areas of abnormal tissue are harder to spot.
The female hormone oestrogen can sometimes stimulate breast cancer cells and their proliferation.The risk of developing breast cancer may rise slightly with the amount of oestrogen a body is exposed to.
3.2 Lifestyle factors (Reversible Causes)
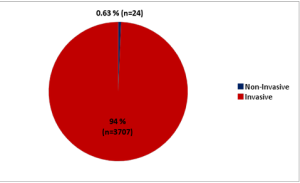
Fig.4
Fig.5
Stages in Cancer
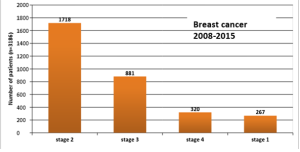
Fig.6
You may see from the Fig. 5 maximum no. of the Breast cancer patients registered with this Institute are in Stage II where the survival is very good.
Cancer stage is based on four characteristics and is based on the results of tests that are done on the tumor and lymph nodes removed during surgery and on other tests.
“Locally advanced” or “Regionally advanced” is a commonly used term to describe the large tumors that involve the breast skin, underlying chest structures, changes to the breast’s shape, and lymph node enlargement that is visible or that a doctor can feel during an exam.
The stage of breast cancer is the key factor in making decisions about the treatment options. If the stage is advance, more treatment is required. But other factors can also be important, such as:
Stage 0 means that the cancer is restricted to the inside of the milk duct and is non-invasive.
Treatment for stages I to III breast cancer usually includes surgery and radiation therapy, often along with chemo or other drug therapies either before or after surgery.
Stage I: These breast cancers are still relatively small and either have not spread to the lymph nodes or have only a tiny area of cancer spread in the sentinel lymph node (the first lymph node to which cancer is likely to spread).
Stage II: These breast cancers are larger than stage I cancers and/or have spread to a few nearby lymph nodes.
Stage III: These tumors are larger or are growing into nearby tissues (the skin over the breast or the muscle underneath), or they have spread to many nearby lymph nodes.
Stage IV (metastatic breast cancer) : Stage IV cancers have spread beyond the breast and nearby lymph nodes to other parts of the body. Treatment for stage IV breast cancer is usually a systemic (drug) therapy.
Inflammatory breast cancer
Inflammatory breast cancer (IBC) can be either stage III or stage IV, depending on whether it has spread to other parts of the body. Treatment for IBC can include chemo or other systemic therapies, local therapies such as radiation, and surgery.
Recurrent breast cancer
Cancer is called recurrent when it comes back after treatment. Recurrence can be local (in the same breast or in the surgery scar), regional (in nearby lymph nodes), or in a distant area. Treatment for recurrent breast cancer depends on where the cancer recurs and what treatments you’ve had before.
Triple-negative breast cancer
Triple-negative breast cancer cells don’t have estrogen or progesterone receptors and also don’t have too much of the protein called HER2. Triple-negative breast cancers grow and spread faster than most other types of breast cancer. Because the cancer cells don’t have hormone receptors, hormone therapy is not helpful in treating these cancers. And because they don’t have much HER2, drugs that target HER2 aren’t helpful, either. Chemotherapy is usually the standard treatment.
The specimen of surgery or biopsy are tested to see if there are estrogen or progesterone receptors. When the hormones estrogen and progesterone are attached to these receptors, they escalate the growth of cancer. Breast Cancers may be called hormone receptor-positive or hormone receptor-negative based on whether or not they have these receptors (proteins). It is important to know the hormone receptor status as it plays a significant role in the treatment of breast cancer. This is done through immunohistochemistry.
Breast cancer cells may have one, both, or none of these receptors.
If breast cancer has one or both of these hormone receptors, hormone therapy drugs can be used to either lower estrogen levels or stop estrogen from acting on breast cancer cells. This kind of treatment is helpful for hormone receptor-positive breast cancers, but it doesn’t work on tumors that are hormone receptor-negative (both ER- and PR-negative).
Based on these tests, breast cancer is described as one of the following types:
This information helps the doctor decide which treatments will work best for the cancer.
The chance of recovery and treatment options depends on the following aspects: (summarize)
Reference:
________________________________________________________________________________
Exercise boosts the immune system and helps to keep weight in check. With as little as three hours of exercise per week, or about 30 minutes a day, a woman can begin to lower her risk of breast cancer. This doesn’t require going to a gym either. Speed or Power walking is more than sufficient!
There is an increased risk of breast cancer for women who have been using birth control pills for more than five years. However due to the low amount of hormones in birth control pills today, the risk is relatively small. But if a young woman has a significant family history of breast cancer, her gynecologist may recommend taking a break for a year from the pill at the 5-year time frame then resuming again for another 5 years. Although evidence-based research data does not offer strong support for this standard of care, it has nevertheless become an increasingly common practice.
Yes, there is. HRT was added to the carcinogenic list by the American Cancer Society in the early 2000s. It is recommended that women with known risks not be placed on HRT to control of menopausal symptoms. They should instead seek other safer alternatives.
Although women who have a family history of breast cancer are in a higher risk group, most women who have breast cancer have no family history. Statistically only 5-10% of individuals diagnosed with breast cancer have a family history of this disease.
Mammography does compress the breasts and can sometimes cause slight discomfort for a very brief period of time. Patients who are sensitive should schedule their mammograms a week after their menstrual cycle so that the breasts are less tender. Ther doctor may say it is fine to take acetaminophen an hour before the x-ray is performed to prevent discomfort too.
Just like with other kinds of cancer, doctors use a rating scale to describe the seriousness, or stages, of breast cancer. There are five stages: 0, I, II, III and IV. In general, the lower the stage, the better the chances for a cure and long-term survival. The stages are based on the size of the tumor, how the cancer affects the underarm lymph nodes and whether the cancer has metastasized, or spread, to distant parts of the body. Treatment during each stage depends on a patient’s individual situation.
Some studies have found that breastfeeding may reduce the risk of breast cancer. The benefit appears to be related to how long the woman breastfeeds.
This question runs through most minds when there is a family history of breast cancer. When a first degree relative (such as a parent or a sibling) is diagnosed with breast cancer, this becomes positive family history and is considered a risk factor. Having said that, the vast majority of breast cancer cases are sporadic; only 5-10% breast cancers are considered to be hereditary and caused by genes passed down from one generation to the next.
A genetic counselor will take into account your family history and other risk factors to give you a better assessment. There are a few signs of genetic breast cancer that are important:
– Early onset breast cancer (< age 50 years)
– Bilateral breast cancer (cancer in both right and left breast)
– Relatives with breast cancer (maternal AND paternal relatives)
– Family history of other cancers (such as ovarian, thyroid, skin, sarcoma, colon, etc.)
Most cases of inherited breast cancer are associated with abnormalities in 2 genes – BRCA1 (BReast CAncer gene 1) and BRCA2 (BReast CAncer gene 2). Everyone has these 2 genes as their job is to suppress tumors in breast and other tissues. When these genes have abnormal changes and are passed down from one generation to the next, they aren’t able to do their job of suppressing tumors effectively, and this increases the risk for cancer. Abnormal changes in BRCA genes account for 1 out of every 10 cases (10%) of breast cancer. An abnormal BRCA gene confers an increased risk – not a diagnosis – of breast cancer. Not everyone who has a BRCA gene abnormality will go on to develop breast cancer, and individuals without BRCA abnormalities may also develop breast cancer.
Studies have shown that, of the 5-10% inherited breast cancers, certain variations in DNA called SNPs (single nucleotide polymorphisms) account for a significant contribution to a higher risk for breast cancer. Other genes involved are TP53, PTEN, ATM, STK11, etc. Genetic counselors are experts in medical genetics and can evaluate family history to determine the most appropriate genetic test, if applicable, and help you decide if genetic testing is right for you or not.
Breast Cancer

Breast Cancer

Breast Cancer




