RGCIRC Team
Colorectal Cancer
27 November, 2023
‘Cancer’, a single word that may send chills down your spine; a malicious disease looked upon with panic, fear and anxiety. As the number of people plagued by this disease is on the rising curve, so are the cancer diagnosis and treatment facilities which are steadily undergoing a sea of changes. While the masses know much about the disease, the awareness about effective disease management, treatment and most importantly the preventive measures is still scanty. Furthermore, when it comes to the cancer of colon and rectum, the situation is all the more hesitant and baffled. Dissemination of the knowledge of colorectal cancer prevention, associated risk factors, tracing the disease at an early stage for efficiently curbing this disease, is the need of the hour. This is the reason that RGCIRC has dedicated this site for creating awareness among the people about colorectal cancer, reinforced by certain common facts and trends observed in the hospital for the past five years.
Colon (commonly called large intestine) is the largest part of our gastrointestinal tract. It is a long, tubular organ, constitutively working along in a niche of gut flora, performing the downstream function of reabsorbing back water and minerals from the digested food into the blood. The remnants are further stored in the rectum and are finally eliminated from the body via anus. Both colon and rectum are deep seated organs and are much neglected and taken for granted, as any other internal part of human body. Cancer develops when the cells in the inner walls of colon/ rectum divide in an unregulated mode to give rise to polyps, which further with time undergoes a series of oncogenic transformations to form cancerous tumors. Colorectal cancer cells are slow growing and the process of change from potentially harmless, yet aberrant pre-cancerous polyps to life threatening cancerous tumors may take years. This gives ample time to treat and nip off the benign polyps at an early stage, before they turn cancerous.
Globally cancer of colorectal cancer is the third most common cancer, affecting both men and women (GLOBOCAN 2012), with a more likelihood in men than in women. In India, colorectal cancer ranks eighth among all other cancer types, the annual incidence rate on an average being 4.2/ 1 lakh population. Though this cancer is more common in the developed countries, but a disturbing facet is its rising trend in India. This feature has been recapitulated at our tertiary cancer centre at Rajiv Gandhi Cancer Hospital and Research Centre (RGCIRC). Five year data (2012-2016) (please refer Figure 1) clearly indicates a steep rise (by 62%) in the number of patients diagnosed with colorectal cancer at RGCIRC.
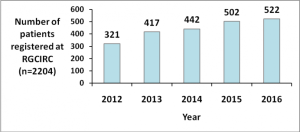
Figure 1. Total number of colorectal cancer patients registered at RGCIRC (2012-2016):
5% of colorectal tumors are hereditary, the rest are sporadic in origin with no major hard and fast determinants. However, increasing evidence suggest certain associated risk factors which can make you more prone to develop this cancer. These factors are:
3.1. Age: Colorectal cancer is mostly presented at an advanced age. The five year data from our institute (Figure 2) also shows that the number of colorectal cancer patients diagnosed is increasing with age, it peaks up in the age group of 51-60 years and eventually decline.
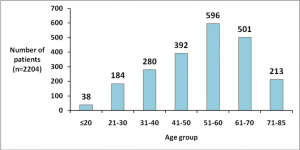
Figure 2. Age- wise stratification of the patients (RGCIRC: 2012-2016):
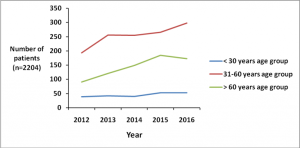
Figure 3. Trend of colorectal cancer in various age-groups (RGCIRC: 2012-2016):
Yet, an alarmingly latent trend could be noted in the middle (30-60 years) age group. It is seen (Figure 3) that the incidence of colorectal cancer is rising in the younger generation. This is an age when an individual is primed to achieve the maximum in his/ her workforce to support a family and come up in life. It is considerably disheartening to note that cancer in this productive age group is witnessing a sudden rise. Precocious nature of colorectal cancer development raises serious concern. This calls for colorectal cancer screening at an early age to reduce the severity associated with this cancer.
3.2. Gender: Colorectal cancer afflicts more males than the females. As is evident from the pie chart (Figure 4), the number of male patients diagnosed with colorectal cancer outnumbers the female number. Our data shows that men have comparatively higher risk (1.5 times) of developing colorectal cancer than women. An unbalanced life style habits in males or less number of female patients coming for treatment (in male dominated Indian society, where females are many a times neglected) could also be a probable reason behind this contradistinction.
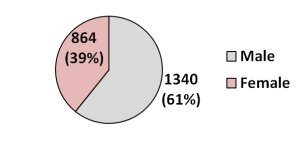
Figure 4. Gender-wise distribution of colorectal cancer cases at RGCIRC (2012-2016):
3.3. Diet and colorectal cancer:
Growing body of evidence suggest that a diet rich in fats and processed red meat predisposes people to colorectal cancer. Red meat includes beef, pork, lamb, liver, etc., the consumption of which may put you at an enhanced risk of developing colorectal cancer. On the contrary, a diet rich in vegetable, fruits, fibers and whole grains help to reduce the risk of colorectal cancer. A fibrous diet aids in concrete bolus formation, which is readily excreted out from the body, without the risk of formation of potentially lethal carcinogens within the body. So it’s better to go for a vegetarian diet and reduce the intake of junk and processed food to keep many lifestyle associated diseases, including colorectal cancer at bay.
3.4. Smoking, use of tobacco products and alcohol consumption:
Smoking, use of tobacco product or heavy alcohol consumption has been linked to the development of many forms of cancer, including colorectal cancer (established by American Cancer Society).
3.5. Genetic makeup:
A known genetic mutation in the APC, MYH, MLH1, MSH2, MSH6, or PMS2 gene in a family member, increases your risk to develop colorectal cancer. A close family person suffering from Familial Adenomatous Polyopsis Syndrome (FAP) is another recognized risk factor. Such individuals are highly recommended to go for genetic screening procedures as per the advice of your treating doctor.
3.6. Physical inactivity:
‘All work and no play makes jack a dull boy’. The same proverb is applicable for lifestyle associated diseases and colorectal cancer. A sedentary life style is associated with increased risk of colorectal cancer. Regular exercise and maintaining a healthy weight diminishes your chance of developing this fatal cancer.
3.7. Having diabetes:
Increasing evidence suggest that Type 2 diabetes mellitus is linked to increased risk of developing colorectal cancer (Yuhara H. et al., Am J Gastroenterol 106(11) (2011): 1911-1921). Both colorectal cancer and Type 2 diabetes share certain common etiological features. A condition of hyperinsulinemia due to diabetes may create a colonic microenvironment that favors development of polyps and further colorectal cancer (American Cancer Society).
Five year data studied at RGCIRC is in agreement with this finding. The pie chart (Figure 5) depicts that among all the co-morbidities it is Type 2 Diabetes mellitus which is most commonly found associated with development of colorectal cancer. This warrants the need for early screening of the individuals suffering from diabetes to negate the possibility of developing colorectal cancer in future.
A history of ulcerative colitis and prostate cancer are among the other well established associated risks of developing colorectal cancer.
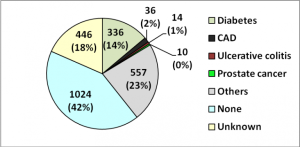
Figure 5. Comorbidity in colorectal cancer patients (RGCIRC: 2012-2016):
Please don’t neglect and consult a doctor immediately if you are persistently experiencing one or more of the above symptoms.
However, colorectal cancer is asymptomatic at early stage and thus may escape early signs and symptoms. This calls for being all the more vigilant and be prepared for undertaking routine screening tests, so as to handcuff the disease at an early stage and treat it appropriately.
One or more of the following methods may be used for screening and detecting colorectal cancer:
Tumor histopathology is well-validated tool employed in cancer hospitals which aids in determining the nature of cancer, its spread to lymph nodes, and many other vital parameters. In histopathology, a small part of cancer tissue is removed at the time of diagnosis by colonoscopy/ sigmoidoscopy or obtained from surgically resected tumor for pathological review and histopathological confirmation. This helps in pathologically classifying the tumor for further deciding definite treatment plans.
As depicted in the pie-chart (Figure 6), Adenocarcinoma is the most common form of colorectal cancer. These adenocarcinomas originate from the glandular epithelial cells of mucus which lubricates the colon and rectum. Other forms include Mucinous Adenocarcinoma, Signet Ring Cell Carcinoma and Squamous Cell Carcinoma.

Figure 6. Histopathological classification of colorectal tumors (RGCIRC: 2012-2016)
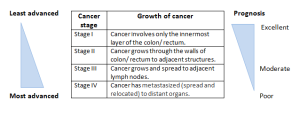
Cancer stage is an important factor which indicates the extent of spread of the tumor which further determines the treatment options and curative aspects. Colorectal cancer is primarily graded as stage I, II, III and IV. Scope for cure and overall survival are both inversely proportional to the progressing stage of the tumor. The table below will briskly familiarize you to the current staging system.
The chances of cancer recurrence and death due to cancer are directly related to the stage of diagnosis. A relook into the data presented at RGCIRC is alarming. As it is clear from the Figure 7, the number of cancer patients diagnosed with late stage of colorectal cancer is increasing. This cancer is being mostly detected at a late stage (stage III and stage IV). Whereas, cancer traced at an early stage shows better survival prospects. The five year data at RGCIRC (Figure 8) shows that there has been no decline in the detection of late stage colorectal cancer, despite the increasing access to cancer related information in general. Therefore, there is a pressing need for improving public awareness for early screening of colorectal cancer at an early stage, for suitable therapeutic interventions.
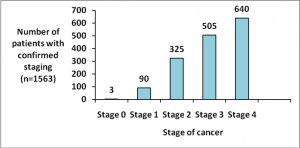
Figure 7. Stage of diagnosis (RGCIRC: 2012-2016):

Figure 8. Year-wise stratification of cancer stage at the time of diagnosis (RGCIRC: 2012-2016):
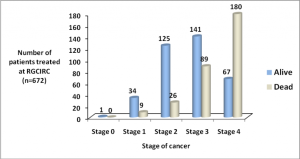
Figure 9. Follow up status of the patients who have taken treatment at RGCIRC (2012-2016):
The follow-up information of the patients who have been treated at RGCIRC (Figure 9), clearly shows that the survival is better for colorectal cancer patients diagnosed at stage I and II, it is intermediate for stage III, whereas survival is worst for stage IV patients. This strongly reiterates that cancer when detected at early stage shows substantially better survival. According to the literature, the 5-year survival for cancer in situ, and stage I and stage II colorectal cancer is as high as 90%, for stage III it is 70%, while for stage IV it is less than 13%. Early screening for colorectal cancer is thus highly recommended so as to enhance once chance of survival.
A multidisciplinary approach is employed for the treatment of colorectal cancer. Surgery, chemotherapy and radiotherapy are the three nodal modalities which may cure or manage cancer. Targeted therapies and immunotherapy are among the upcoming therapeutic avenues which can efficiently treat certain kinds of tumor. Depending upon your tumor size, type, location, extent of disease and your health condition your Doctor will treat you by one or more of these methods. For early stage, less advanced, operable tumors, surgical resection is performed. But when the tumor becomes inoperable, or when it spreads to the lymph nodes, your Doctor may resort to chemotherapy and surgery. However, when the tumor has metastasized (Stage IV), palliative chemotherapy is given with intent to slow down the spread of the disease, or to shrink tumor and alleviate the symptoms and side effects. The aim is to provide good quality of life to the cancer patient.
Radiotherapy use high energy radiations to destroy cancer cells. Radiotherapy is given under limited conditions in colorectal cancer. It is often given for the cancer of the rectum. This is because rectal tumors owing to their location, surgical resection becomes relatively difficult. In these tumors, radiotherapy is first administered to shrink the tumor for the ease of surgical resection. Alternatively, it is also given after surgery to remove any residual cancer cells lining the internal organs. Radiotherapy is also given when the patient is in a compromised health situation and is not fit enough for surgery. Palliative radiotherapy is administered in the patients with advanced cancer, as a measure to ease the symptoms and pain caused by intestinal obstruction or when the cancer has spread to bones or brain.
Both chemotherapy and radiotherapy are not specific to cancer cells and affects (kills) both cancer cells and normal cells (to some extent). While chemotherapy destroys all the rapidly dividing cells (which include both cancerous and non-cancerous dividing cells), radiotherapy may affect nearby healthy cells. These cause unpleasant side-effects to the patient. Some of the common side effects of chemotherapy and radiotherapy have been tabulated below:

The severity and extent of these side effects vary widely among the patients. Please, don’t worry too much of these side effects as they are mostly transient and generally lessen and eventually subside after a few days of treatment.
Apart from these modalities of treatment, Palliative/ Supportive care can be taken at any stage of cancer. Nevertheless, it is the only option available to a terminally-ill cancer patient when the cancer is incurable. In supportive care, symptomatic treatment is rendered to improve quality of life of the patient. The aim is to relieve the patient from pain and distress and prolong life. A holistic approach is followed; the patient is counseled and symptoms are pacified.
Even after a successful treatment, the chances of tumor recurrence cannot be negated. The chance of cancer to return back is high during the first few years. Hence, it is advisable to go for routine check-ups and screening to ensure that the tumor has not reappeared or spread. Your blood CEA levels can be tracked if their levels were found high before surgery. CT scan can be performed after one year, thereafter 3 years and then followed up by 5 years; or as per the advice of your treating Doctor’s advice. Also, a cancer of colon/ rectum can make you more prone to develop prostate or uterine cancer. A screening for these cancers is also advisable.
In case your cancer relapses, still it can be treated with intent to cure.
Thus, it can be concluded that even though treatment options are available for colorectal cancer, but prevention is always better than cure. (i) Eating a well-balanced diet rich in vegetables and fibers, (ii) regular exercise and physical activity and (iii) staying away from tobacco and alcohol are three magical mantras that we can do from our side to reduce the risk of colorectal cancer. But these approaches may seem to be non-empirical. On the other hand, controlling the hereditary and genetic factors is beyond our reach, yet these are empirical variables. Colorectal cancer is highly treatable when diagnosed at an early stage. Self-examination and timely screening is the Holy Grail for early detection and cure of this cancer. We Indians, are generally not in a habit of undertaking regular screening tests and examinations, and have a tendency to act only when symptoms become apparent. At times these tests seem to be a costly affair. But time is perhaps more precious than money. The time lost by late detection of colorectal cancer is something which even costly treatments cannot make-up. So let us be watchful and proactive in the fight against this deadly disease. Just like we seek to upkeep our external appearance, it’s time that we take some efforts to care of our gut which indeed is bestowed to perform an important function in the human body.
References:
https://www.medicinenet.com/colon_cancer/article.htm
http://www.icmr.nic.in/guide/cancer/Colorectal/Colorectal%20Cancer.pdf
https://www.cancer.org/cancer/colon-rectal-cancer.html
Ans. Rectal bleeding could be due to many diseases like anal fissures, hemorrhoids (piles), colitis or could be even because of obstruction by colonic polyps. Please consult your Gastroenterologist immediately if you see blood in your stool. While Fecal Occult Blood Test (FOBC) just determines the presence of blood in stool, Colonoscopy or Sigmoidoscopy views the colonic environment. Depending upon your medical condition, your treating Doctor would advise you further in this regard.
Ans. The U.S. Preventive Services Task Force (USPSTF) recommends that adults of age group 50-75 years should be screened for colorectal cancer. But this may not be true for Indians. Observation from our hospital indicates that the incidence of colorectal cancer is increasing in the younger age group. A screening test after 40 years is thus advisable. However, if you have a close relative with colonic polyps, or if you are suffering from Inflammatory Bowel Disease, or Familial Adenomatous Polyposis, an early screening for the detection of colorectal cancer would be all the more beneficial.
Ans. About 5% of colorectal cancers like Hereditary Nonpolyposis Colorectal Cancer (HNPCC) and Familial Adenomatous Polyposis (FAP) are genetic and caused by inherited gene mutations (germline mutations). Such diseases are inherited within the family. Consulting a trained Genetic Counselor, who may ask you a few questions (pedigree analysis) and identify your/ any family member’s chance of developing colorectal cancer, is advisable in such cases.
Ans. CEA (Carcinoembryonic Antigen) is a colorectal tumor marker detected in blood. The normal range is <2.5 ng/ ml (for non-smokers) to <5 ng/ ml (for smokers), while its level rises as cancer progresses. However, testing for CEA in the blood is not a sure-shot test. This is because, not all colorectal cancers show elevated CEA levels. You are advised to keep track of your CEA levels only in case – when their levels were found high before surgery. In such a case, your CEA level should fall after surgery and should ideally not increase, unless the cancer recurs.
Ans. No, it is not advisable to take vaccination in-between your chemotherapeutic schedules. This is because successful vaccination is achieved only when an effective immune response is mounted in the individual. But, chemotherapy kills rapidly dividing cells in the bone marrow, and leaves the patient immunocompromised. Hence, vaccination in between chemotherapy brings no potential benefit. In fact, it may also enhance your chances of infections.
Ans. Alternative medicines like Ayurveda, Homeopathy, Naturopathy, or any other form, may help to lessen pain. However, they are definitely not a cure as they are not clinically tested. Moreover, when such medications are taken along with chemotherapeutic regimens, it can lead to the alternative medicine – drug interaction. This may bring adverse effects and hence is not usually recommended.
Ans. The hair follicle cells are among the fastest dividing cells of the human body. Since chemotherapeutic drugs target rapidly dividing cells in the body, it may harm your hair follicles too. Depending on the type of drug and the dose of the drug administered, you may find thinning of your hair (including eye-lashes or any other part) or even complete hair loss. But please don’t worry too much, as this is just a temporary effect. Your hair starts to re-grow at its normal rate after 3-10 months of chemotherapy.
Ans. Graying of hair is due to stress, and chemotherapy is a stress to the body. Chemotherapy may change the texture, color or the amount of your hair, but not always. It is advisable to use a mild shampoo (free of sodium lauryl sulphate, a known skin irritant) after chemotherapy. Also, avoid coloring/ perming/ straightening your hair before chemotherapy.
Ans. Just after surgery you may find it difficult to resume your normal job routine. Surgical wounds require a few weeks to heal. Cancer may leave you with a feeling of isolation and loneliness. To overcome these emotions, it is perhaps best to resume your routine lifestyle. However, avoid strenuous exercise and driving. Resort to – light activities for 1-4 weeks, followed by moderate level of works for 4-6 weeks and normal activities thereafter. Your treating Doctor would be the best to advise you in this aspect.
Ans. Though supportive/ palliative care can be taken at any stage of cancer treatment, but it assumes much more importance for terminally ill cancer patients. Supportive care aims at relieving suffering and improving quality of life of the patient. It is based on the principles of ethics and holistic care. Rajiv Gandhi Cancer Institute and Research Centre has a separate Department of Palliative Care which provides supportive care to terminally ill cancer patients, at their home, free of cost.

Colorectal Cancer

Colorectal Cancer

Colorectal Cancer




