

Interventional Procedures
Overview
Sentinel Lymph Node Biopsy
Sentinel lymph node mapping and sentinel lymph node biopsy (SLNB) is a minimally invasive technique which allows the surgeon to excise and meticulously examine the primary draining lymph nodes after those have been identified by radionuclide procedure. The principle underlying sentinel node surgery is rooted in the concept that the sentinel node is the first draining lymph node from a tumor and is predictive of lymph nodal metastasis.
The use of radio-nuclide injection close to or into the tumor, nuclear imaging to visualize the sentinel lymphnode, detection and excision with the help of a handheld gamma probe to identify sentinel lymph nodes and its histopathological examination completes the procedure. It is helpful in early breast cancer, head neck and some gynaecological malignancies. SLNB provides more accurate prognostic information for these patients and identifies those patients that may benefit from additional treatment to the lymphatics.
Pharmacological / Physical Stress for Myocardial Scintigraphy
Pharmacological / Physical stress induced myocardial perfusion scintigraphy performed either with a treadmill or post adenosine or dobutamine infusion for evaluation of cardiac disorders. A well qualified cardiologist is involved from the beginning in this intervention for the best possible results.
Thyrogen induced whole body iodine-131 scan or therapy
Thyrogen (Thyrotropin alpha) is a recombinant human TSH can be used for planning of adjuvant radioiodine treatment or follow-up Iodine-131 scan.
State-of the art ‘Theranostic’ Centre
Theranostic has originated by a combination of two words ‘Therapy and Diagnostics’. The term was first coined by John Funkhouser in 1998 when the concept of personalized medicine appeared. In this concept, the same target has been used for the diagnosis and the treatment. An imaging probe is used to image a particular cancer cell antigen. If positive, the same probe labeled with a therapeutic radionuclide is used for subsequent treatment targeting the same antigen. Hence, ‘we treat what we see, and we see what we treat.’ It is a highly personalized treatment concept and secures a high drug delivery level to the target with fewer side effects in normal cells. This concept also holds valid for planning any targeted treatment. Identifying a target before treatment improves selection and hence reduces heterogeneity. This concept is used in all Nuclear Medicine radionuclide therapies.
Radionuclide Therapy
We are doing radionuclide therapy since the inception of the department. We are providing facility for all the approved radionuclide therapies. The Institute has 3 bed dedicated ward for Radionuclide therapy approved by Bhabha Atomic Research Centre (BARC) and Atomic Energy Regulatory Board (AERB), Government of India.
Following radionuclide treatments are being performed on a regular basis in the department:
- High dose Radioiodine therapy for thyroid cancer patients
- Radioactive Iodine treatment for Hyperthyroidism is also performed as an outpatient procedure routinely.
- Lu-177 DOTATATE Peptide Receptor Radionuclide Therapy (PRRT) for Neuroendocrine Tumors.
- Lu-177 PSMA Peptide Receptor Radioligand therapy (PRLT) for Castration Resistant prostate cancer (CRPC)
- I-131 MIBG therapy for neuroendocrine tumors
- Samarium (153.5m), Strontium & Phosphorus (P-32), for bone pain palliation.
- Y-90 trans-arterial radio-embolization (TARE) for HCC and, liver dominant metastasis for other cancers.
- Ac-225 PSMA therapy (Alpha Therapy) for Castration Resistant prostate cancer
Radioiodine Therapy for Thyroid cancer
High dose Iodine-131 treatment for thyroid cancer patients is routinely available. A one-to-one interaction with the Thyroid surgeon is done during planning and performing of the treatment. We have treated more than 2000 thyroid cancer patients successfully.
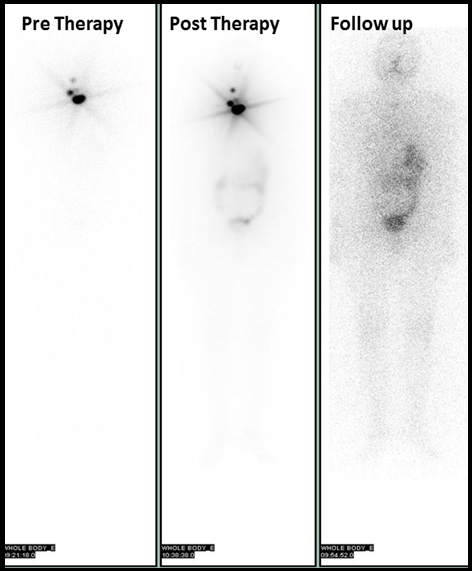
A thyroid cancer patient following surgery, showed few foci of residual thyroid tissue in the neck in pre and post radioiodine therapy scans, which showed complete response in a six months follow-up scan
Peptide Receptor Radionuclide Therapy (PRRT) for Neuroendocrine Tumors
Imaging and treatment of Neuroendocrine tumors (NET) is the example of successful implementation of the theranostic concept and a valid examples of personalized medicine.
Biologically NET’s are functioning or nonfunctioning. The functioning ones are associated with clinical syndrome & increased bio-markers. Nonfunctioning tumors have histopathological (HP) features of NET but no clinical syndromes. These have high expression of somatostatin receptors which have five different G-protein coupled somatostatin receptor sub-types (SSTR 1-5) cloned & pharmacologically characterized. SSTR 2 is expressed in approx. 90% of G-1 NET & 80% of pancreatic NET. In insulinomas, however < 50% expresses SSTR-2.
Histopathological grading also contributes to treatment selection. Well differentiated NET G-1, mitotic count < 2/10 HPF with Ki 67 < 3% & G2: mitotic count 2-20 / 10 HPF with Ki 67 3-20% show good expression of somatostatin receptor and are candidates for receptor based therapy. Even Grade-3 NET may also benefit from radionuclide therapy, provided a DOTANOC PET scan shows good receptor expression.
177Lu DOTATATE therapy can be successfully applied to these patients with excellent results and can prolong survival in metastatic NET which has failed conventional therapy. In selected cases, it has also been used to downstage the tumor, in a neoadjuvant setting, followed by curative surgery.
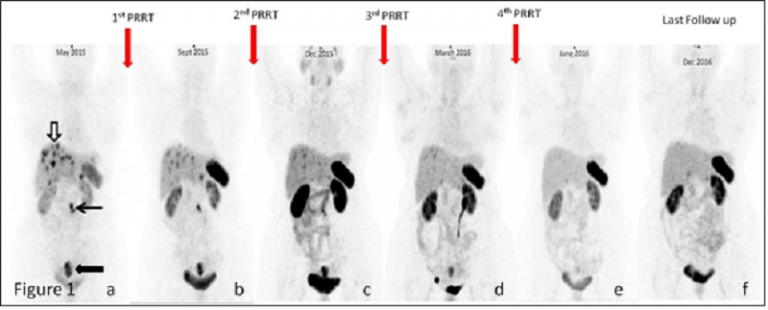
A 63 old lady with grade 1 rectal carcinoma with lymph node and liver metastasis treated with 4 cycles of 177Lu-DOTATATE. Serial 68Ga-DOTANOC PET-CT Maximum intensity projection images (a-f): Image (a) showed strong (more than spleen) somatostatin receptors (SSTRs) expressing rectal lesion (black block arrow), retroperitoneal lymphnodes (black arrow) and liver lesions (empty block arrow). Serial images (b to e) after each peptide receptor radionuclide therapy (PRRT) showed response in liver lesions and retroperitoneal lymphnodes and complete response after four cycles. Last follow up image (f) showed no abnormal SSTRs expressing lesion in the body.
Peptide Radioligand Therapy (PRLT) for Prostate Cancer
It is known that metastatic prostate cancer responds to well established innovative anti androgen treatment. In addition to other conventional treatment methods the recently approved androgen receptor antagonist enzalutamide & CYP17A1 inhibitor abiraterone has been reported to have 3.9 & 4.8 months survival benefit respectively. Progression to androgen independence is the main cause of morbidity & death in these patients. Based on the theragnostic concept, the main aims of treatment are to improve outcomes by early interventions in suboptimal responders sparing patients from over treatment, to reduce acute & late treatment related side effects, achieve best possible therapeutic gain, ensure effective palliation & improve quality of life. Tumor targeting with 177Lu-PSMA has the potential advantage of saving the normal tissue while delivering high dose to tumor, easy radiopharmaceutical labelling & high expression in all cancer cells thus making it an optimal target for radionuclide therapy. It is safe with a low toxicity profile achieving good therapeutic benefit. It has been found to improve survival and quality of life of end stage mCRPC patients. We have also seen objective regression in lesions and symptomatic relief. In our experience at RGCIRC, we have found it to a safe & effective method for treating end stage androgen independent, progressive CRPC, where good receptor expression is demonstrated by Ga-68 PSMA scan before therapy. We have also published our experience in various peer reviewed international journals.
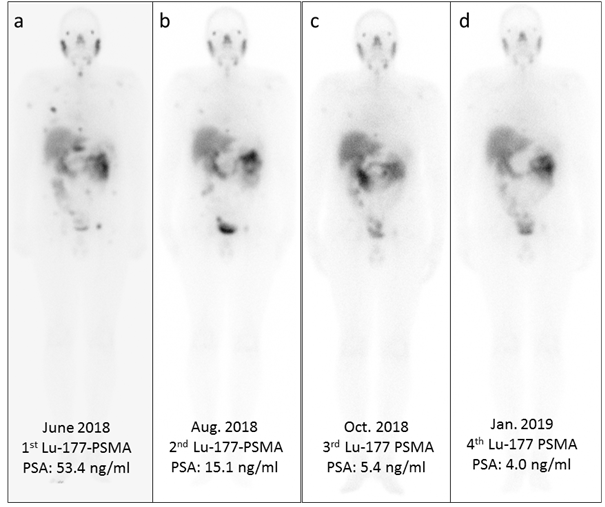
A 68 years old gentleman, known case of Ca prostate on treatment since last ten years. He has received multiple lines of standard treatment and presented with multiple PSMA avid bony and liver lesions. He was treated with four cycles of 177Lu-PSMA and archived good partial response. Anterior planner images (a, b, c, d) 24 hours post Lu-177 PSMA therapy. Serial images following 1st cycle (image a), 2nd cycle (image b), 3rd cycle (image c) and 4th cycle (image d) of Lu-177 PSMA showed >90% decline in PSA and response in all bony lesions sites.