RGCIRC Team
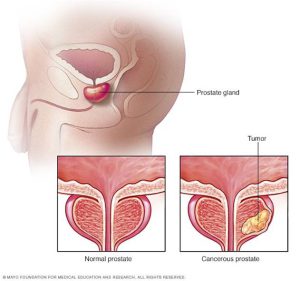
Prostate Cancer
27 November, 2023
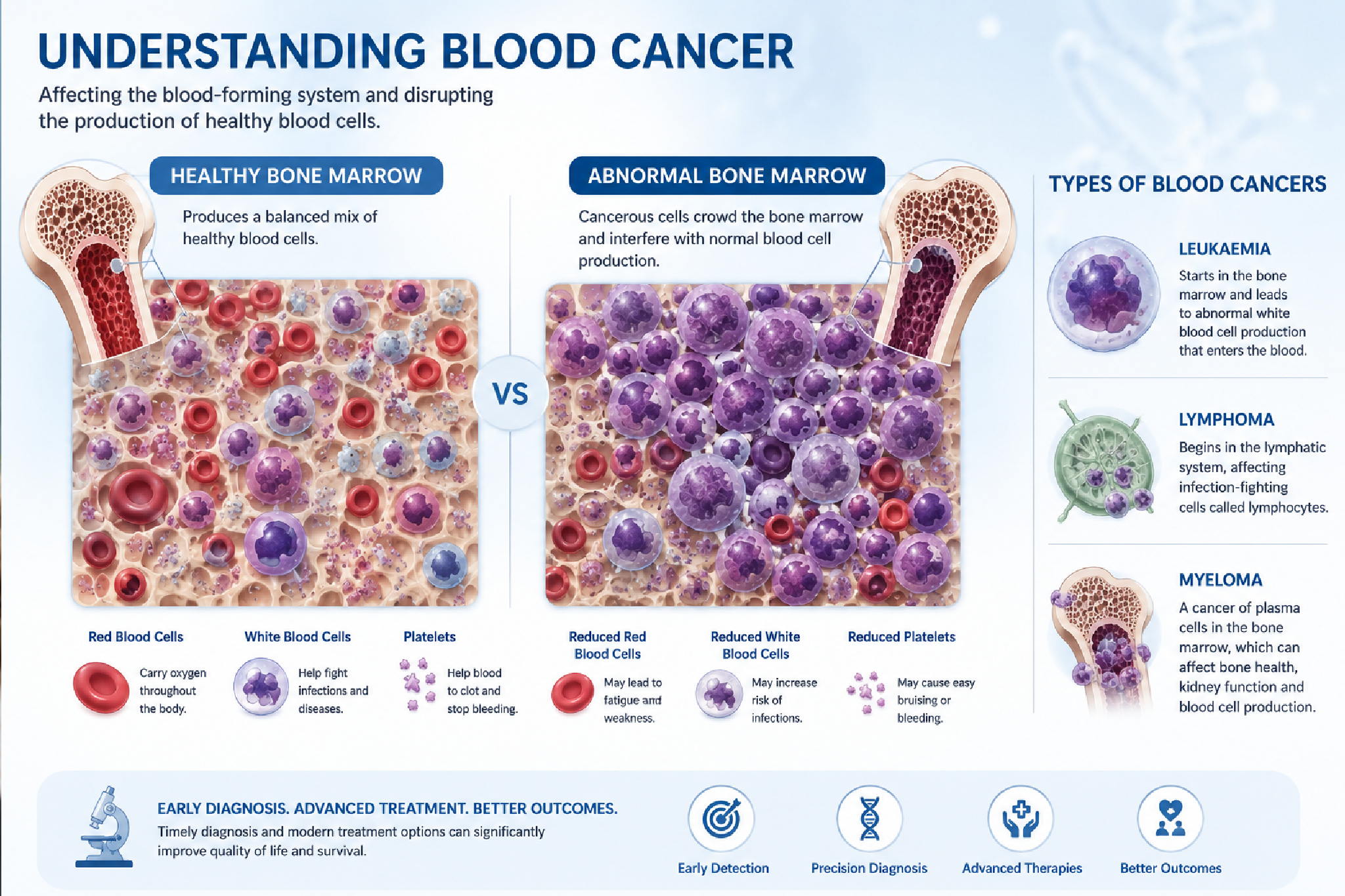
Prostate cancer is the second most commonly occurring cancer in men and the fourth most commonly occurring cancer overall. There were 1.3 million new cases in 2018. As the name suggests, it occurs in prostate — a small walnut-shaped gland in men that produce prostatic secretion, which is necessary to preserve vitality of sperm. This cancer is generally slow growing and the majority of men with low grade prostate cancer live for many years without symptoms and affecting survival of patient, in fact these patients die due to other illness rather than from prostate cancer.
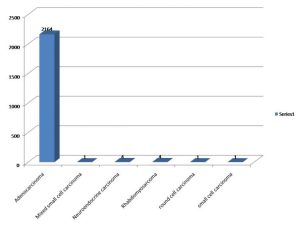
Most men who are diagnosed with prostate cancer have a good chance of recovery. This is because prostate cancer often only grows in the prostate (localized) and do not spread to other parts of the body. But, once prostate cancer begins to grow quickly or spreads, as in high grade disease, it is dangerous. Therefore , appropriate management is the key. This is the reason that RGCIRC has dedicated this site for creating awareness among the people about prostate cancer followed by Breast Cancer and Colorectal Cancer. Here Five-year Data from [2012 to2016][please refer figure 1]clearly indicates steep rise in the number of patients diagnosed with Prostate cancer at RGCIRC .
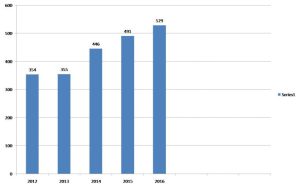
Figure 1. Total number of prostate cancer patients registered at RGCIRC (2012-2016)
It’s still not known what causes prostate cancer, although a number of things can increase the risk of developing the condition. Cancer grows from cells which have acquired mutation or inherited mutation (familial cancer) in their genetic material. Familial prostate cancer occurs in men who have particular genetic mutations, such as genetic mutations seen in some families with breast and ovarian cancer. However, most cancer-causing genetic mutation occurs after birth.
There are some risk factors which may affect one’s chances of developing prostate cancer. These include:
50 years of age. The five year data from our institute [figure 2] also shows that the number of prostate cancer patients diagnosed is increasing with age, it peaks up in the age group of 61-70 years and eventually decline.
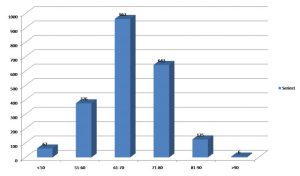
Figure 2.Age-wise stratification of the patients (RGCIRC: 2012-2016)
[Mean age-67.90]
[Median age-68]
Prostate cancer does not cause any symptoms until it has reached a more advanced stage or significantly increased in size. It may then cause problems such as
Most Prostate Cancers are first suspected during screening with a prostate specific antigen (PSA) blood test or digital rectal exam (DRE).Most men without prostate cancer have PSA levels under 4ng/ml of blood. The chance of having prostate cancer goes up as the PSAlevel goes up. Normal PSA level chart according to age given below.
| Age | Asian Americans | African Americans |
| 40-49 | 0-2.0ng/ml | 0-2.0ng/ml |
| 50-59 | 0-3.0ng/ml | 0-4.0ng/ml |
| 60-69 | 0-4.0ng/ml | 0-4.5ng/ml |
| 70-79 | 0-5.0ng/ml | 0-5.5ng/ml |
PSA test is also an important part of monitoring prostate cancer during and after treatment. If certain symptoms or the result of tests such as PSA blood test or DRE suggest that you might have prostate cancer, your doctor will do a prostate biopsy. A biopsy is a procedure in which small samples of the prostate are removed and then looked at under a microscope. There are two types of biopsy; Trans rectal ultrasound (TRUS) guided and MRI–TRUS fusion guided biopsy.
TRUS guided approach is more commonly used to take prostate biopsy, as we get patients with high PSA usually. Whereas, MRI-TRUS fusion guided biopsy is indicated when PSA is not very high but there is suspicion of disease in MRI prostate, or if PSA is high but previous TRUS guided biopsies were negative. Multi-parametric MRI has been used to assess the prostate for presence of suspicious nodule of cancer. The system for evaluating multi-parametric MRI is called PI–RADS [the prostate imaging reporting and data system]. It’s a structured reporting scheme for evaluating the prostate for prostate cancer, the score is;
MRI-TRUS fusion guided biopsy is indicated if PIRADS is ³ 3.
Gleason Scoring
Prostate cancer is also given a grade on microscopic examination called a Gleason score. This score is based on how much the cancer looks like healthy tissue when viewed under a microscope. Less aggressive tumors generally look more like healthy tissue. Tumors that are more aggressive are likely to grow and spread to other parts of the body. They look less like healthy tissue.
The Gleason system is used to grade prostate tumors from 2 to 10, where a Gleason score of 10 indicates the most aggressive tumor. The pathologist assigns a number from 1 to 5 for the most common pattern observed under the microscope and then does the same for the second most common pattern. The sum of these two numbers is the Gleason score.
Grade Group
Tumor Histopathology
Imaging
MRI pelvis is used for local staging i.e. to look for local spread of disease. CECT (abdomen, and chest) with Bone scan were being used for systemic staging i.e. to see for distant spread of disease. Now a day, PSMA-PET scan is emerging as a one stop shop for evaluation for distant spread of disease, with very high accuracy.
Regardless of which diagnostic tests were used, your doctor will review your test results with you and discuss what the next steps will be depending on stage of disease.
Staging in cancer is done to describe Local and systemic spread of cancer.
TNM stages
The TNM staging system stands for Tumor, Node and Metastasis.
The most important distinction made by any staging system is whether or not the cancer is still confined to the prostate. In the TNM system, clinical T1 and T2 cancers are found only in the prostate, while T3 and T4 cancers have spread beyond prostate.
Stage 1 prostate cancer is characterized by a Gleason Score of less than 6. The Cancer is restricted to one half of the prostate with no spreading to surrounding tissues and a PSA level below 10.
Stage 2A
In stage 2A prostate cancer, the tumor is still restricted to one side of the prostate, but the Gleason score may be up to 7, and the PSA levels are greater than 10 but less than 20 ng/mL.
By stage 2B, the tumor may have spread to the opposite side of the prostate gland, but it also may still be contained on one side. If the tumor is still restricted to one half of the prostate, a Gleason score of 8 or higher or a PSA level of 20 or greater categorizes the cancer as stage 2B.
If the tumor has spread to both sides of the prostate then the stage is 2B regardless of the Gleason score and the PSA level.
Stages 3 and 4
By the time prostate cancer has reached stage 3 or stage 4, the cancer is very advanced. At this point, the stage is determined by the extent of the spread of the cancer, and the PSA level and Gleason score do not factor in the staging.
In stage 3 the tumor has grown through the prostate capsule and may have invaded nearby tissue. By stage 4 the tumor is fixed or immovable and invades nearby structures beyond the seminal vesicles. It may also have spread to distant sites like lymph nodes or bones.

The chances of cancer recurrence and death due to cancer are directly related to the stage of disease at diagnosis. As, cancer treated at an early stage shows better survival prospects. Figure 3, shows the distribution of prostate cancer patients according to their stage of disease. The number of cancer patients diagnosed with late stage (stage III & stage IV) has highest share. The five-year data at RGCIRC (figure3) shows that there has been no decline in the detection of late stage prostate cancer, despite the increasing access to cancer related information in general. Therefore, there is a pressing need for improving public awareness for early screening of prostate cancer at an early stage, for suitable therapeutic treatments.
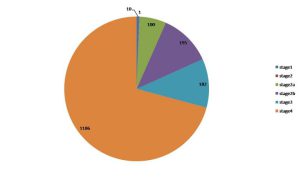
Figure 3. Stage of disease at diagnosis (RGCIRC: 2012-2016)
Local treatments get rid of cancer from a specific, limited area of the body. Such treatments include surgery and radiation therapy. For men diagnosed with early-stage Prostate cancer, local treatments may get rid of the cancer completely. If the cancer has spread outside the prostate gland, other types of treatment called systemic treatments may be needed to destroy cancer cells located in other parts of the body.
The type of surgery depends on the stage of the disease, the man’s overall health, and other factors.
Surgical options include:
Radical (open) prostatectomy: A radical prostatectomy is the surgical removal of the Entire prostate and the seminal vesicles. Lymph nodes in the pelvic area may also be removed. A side effect of this operation has the risk of affecting sexual function and urinary incontinence. Nerve-sparing surgery, when possible, increases the chance that a man can maintain his sexual function after surgery by avoiding surgical damage to the nerves that allow erections and orgasm to occur. Patient may also require medicine for penile rehabilitation, till his erection does not recover. Patient might require injection of debulking agents, artificial urinary sphincter implantation for post prostatectomy urinary incontinence, but in more than 95% patients continence recover within 1 year.
Robotic or laparoscopic prostatectomy: This type of surgery is possibly much less invasive than an open prostatectomy and may shorten recovery time. It causeless bleeding and less pain, but the sexual and urinary side effects can be similar to those of a radical (open) prostatectomy. In the last 10 years, laparoscopic (Robotically Assisted) radical prostatectomy has become very popular and replaced open radical prostatectomy.
Bilateral orchiectomy: Bilateral orchiectomy is the surgical removal of both testicles, indicated for metastatic disease, or for locally and locally advance disease, if patients life expectancy is less than 10 year.
Radiation is the strategic use of ionizing radiation or photons to kill cancer cells. The targeted cells die without growing or replicating themselves. Radiation therapy, like surgery, is very effective at killing localized or locally advanced prostate cancer and has the same cure rate as surgery.
The types of radiation therapy used to treat prostate cancer include:
I. External Beam Radiation Therapy (EBRT)
EBRT is the most common type of radiation therapy. The radiation oncologist uses a Machine located outside the body to focus a beam of X-rays on the area with the Cancer.
Different types of EBRT treatments are,
1 Conventional
2 Moderate hypo-fractionation
3 Ultra-hypo-fractionation
II. Brachytherapy [Internal Radiation Therapy]
Internal radiation therapy is the insertion of radioactive sources directly into the Prostate. Brachytherapy involves placing radiation therapy “seeds” or temporary catheters inside the prostate that emit radiation at a very short distance.
Hormone therapy is also called androgen deprivation therapy (ADT) or androgen Suppression therapy. The goal is to reduce levels of male hormones, called androgens, in the body, or to stop them from affecting prostate cancer cells.
Primary hormone therapy
Since testosterone serves as the main fuel for prostate cancer cell growth, it’s a common target for treatment. Primary hormone therapy [androgen deprivation therapy or ADT] is part of the standard of care for advanced metastatic prostate cancer.ADT is designed to either stop testosterone from being produced or directly block it from acting on prostate cancer cells.
The majority of prostate cancer cells will die or stop growing once they are deprived of testosterone. However, in many men, some cells gain the ability to grow in the low-testosterone environment created by hormone therapy. As this hormone therapy-resistant prostate cancer cells continue to grow, primary hormone therapies have less and less of an effect on the growth of the tumor over time. This state is also referred to Castration-resistant prostate cancer (CRPC).
Hormone therapy is often given together with radiation therapy for localized disease and locally advances disease – it is also used alone or in combination with other treatments for men with metastatic prostate cancer.
The decision on when to start chemotherapy is difficult and highly individualized based on several factors.
Many men who are suffering from their cancer will experience symptomatic improvement after starting chemotherapy. For example, pain is often reduced in men starting docetaxel, and quality of life is generally better for men with cancer-related symptoms who receive chemotherapy as compared with no therapy.
Currently, taxane chemotherapy, given with prednisone, is the standard of care for men with metastatic prostate cancer that has spread and is progressing despite hormone therapy. Taxane chemotherapy agents include docetaxel and cabazitaxel.
Taxane chemotherapy is also effective in prolonging life in patients who have a high burden of cancer on scans when starting hormonal therapy for the first time for metastatic disease.
Platinum-based chemotherapy agents including carboplatin, cisplatin, and oxaliplatin are used for the treatment of various cancer types. It is sometimes used in very advanced prostate cancer patients who have exhausted all other treatment options or in patients who have rare subtypes of prostate cancer.
Rajiv Gandhi Cancer Institute & Research Centre continues to be the preferred Centre for prostate cancer treatment in India. Our Department of Uro-Oncology opened its doors in 1996 with a handful of conventional open surgeries with Laparoscopic and Robotic Uro-oncoprocedures. Our approach to prostate cancer management is based on multiple factors, such as presentation stage, age, and health status of the patient. Conventionally, we comply with the proven modality of expectant management, patient observation and active surveillance. The five-year data at RGCIRC (figure 5) shows that 52% of total patients took treatment from our institute and the rest of (48%) patients came here for diagnosis, second opinion and follow up.
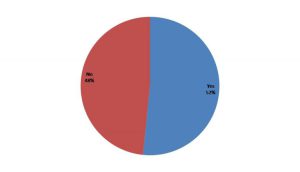
Figure 5. Status of the patients who have taken treatment or not at RGCIRC (2012-2016)
The five year data at RGCIRC (figure6) shows that 366 cases treated by Surgery; 59 were treated by Chemotherapy; Radiotherapy was given to 49 cases; Hormone therapy was given to 234 cases; 150 cases treated by combination of Surgery and Hormone; 75 Cases treated by combination of Hormone and Radiation; 11 Cases treated by combination of Surgery, Chemotherapy and Radiation therapy.11Cases treated by combination of Surgery, Chemotherapy, Hormone therapy and Radiation Therapy. Rest of 1052 patients came here for Second opinion, Diagnosis and Follow up.
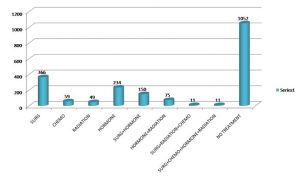
Figure 6.Analysis of Treatment Modalities at RGCIRC (2012-2016)
FOLLOW-UP AND ROUTINE CHECK –UP
After treatment for prostate cancer, follow-up care is important to help maintain good health, manage any side effects from treatment, watch for signs that the cancer has come back after treatment, and screen for other types of cancer. A follow-up care plan may include regular physical examinations and other medical tests to monitor your recovery during the coming months and years.
Men recovering from prostate cancer are encouraged to follow established guidelines
For good health, such as reaching and maintaining a healthy weight, exercising, not
Smoking, eating a balanced diet, and following cancer screening recommendations.
Here are general recommendations for men recovering from prostate cancer:
In addition to regular physical examinations, the following tests are recommended to monitor for a prostate cancer recurrence:
>> PSA TEST
>>DIGITAL RECTAL EXAM [DRE]
A doctor uses this test to identify abnormalities or changes in the prostate by feeling the area using a finger.
References:
>>www.cancer.Net/prostate cancer
>>Prostate cancer foundation patient guide
>>www.cancer.org/prostate cancer
>>American Cancer Society
Ans: Prostate cancer begins when cells in the prostate gland start to grow uncontrollably. The prostate is a gland found only in males. It makes some of the fluid that is part of semen. Prostate cancer is one of the most common types of cancer in men.
Ans: It’s not clear what causes prostate cancer. Doctors know that prostate cancer begins when some cells in your prostate become abnormal. Mutations in the abnormal cells’ DNA cause the cells to grow and divide more rapidly than normal cells do. The abnormal cells continue living, when other cells would die. The accumulating abnormal cells form a tumor that can grow to invade nearby tissue. Some abnormal cells can also break off and spread (metastasize) to other parts of the body.
Ans: Prostate cancer may cause no signs or symptoms in its early stages.
Prostate cancer that’s more advanced may cause signs and symptoms such as:
4. What are the risk factors For Prostate Cancer?
Factors that can increase your risk of prostate cancer include:
Age. Your risk of prostate cancer increases as you age.
Race. For reasons not yet determined, black men carry a greater risk of prostate cancer than do men of other races. In black men, prostate cancer is also more likely to be aggressive or advanced.
Family history. If men in your family have had prostate cancer, your risk may be increased. Also, if you have a family history of genes that increase the risk of breast cancer (BRCA1 or BRCA2) or a very strong family history of breast cancer, your risk of prostate cancer may be higher.
Obesity. Obese men diagnosed with prostate cancer may be more likely to have advanced disease that’s more difficult to treat.
5. Is Family History Important?
Yes.
6. Who should be screened for Prostate cancer?
PSA screening generally encourage the test in men between the ages of 50 and 70, and in men with an increased risk of prostate cancer.
7. What are the screening tests for cancer?
The PSA test isn’t the only screening tool for prostate cancer. Digital
Rectal examination (DRE) is another important way to evaluate the
Prostate and look for signs of cancer.
8. If I have Prostate Cancer, should I see an oncologist or Urologist for the treatment?
Oncologist
9. What is active surveillance?
Active surveillance is a way of monitoring prostate cancer that hasn’t spread outside the prostate (localized prostate cancer), rather than treating it straight away. You might hear it called active monitoring. Many men on active surveillance won’t need treatment in their lifetime.
The prostate is close to several vital structures, prostate cancer and its treatments can disrupt normal urinary, bowel, and sexual functioning. This section discusses side effects that might be experienced as well as advice on managing those side effects.
Urinary Dysfunction: The term urinary dysfunction encompasses both urinary incontinence, which can range from some leaking to complete loss of bladder control, and irritative voiding symptoms (symptoms triggered by the irritation of the tissues), including increased urinary frequency, increased urinary urgency, and pain upon urination.
Bowel Dysfunction: Solid waste that is excreted from the body moves slowly down the intestines, and, under normal circumstances, the resultant stool exits through the rectum and then the anus. Damage to the rectum can result in bowel problems, including rectal bleeding, diarrhea, or urgency.
Erectile Dysfunction: Regardless of whether the nerves were spared during surgery or whether the most precise dose planning was used during radiation therapy, erectile dysfunction remains the most common side effect after treatment.

Prostate Cancer
Prostate Cancer
Prostate Cancer